by Hans Werner
Department of History, University of Winnipeg
and Jenifer Waito
Department of Education, University of Winnipeg
|
By 1895, the process of medicalizing childbirth was well underway in North America. It was characterized by an increase in physician-attended births, increased reliance on medical technology and science, and a slow but steady decline in midwifery. In fact, by the end of the nineteenth century, it was becoming the norm for physicians to attend to birthing women. [1] The increase in physician-attended births is directly correlated to the steady decline of popularity and numbers of midwives at that time. However, the practice of midwifery did not disappear uniformly across all strata of society. As Wendy Mitchinson suggests, the few remaining midwives that held out against the increasing domination and authority of the medical profession remained active in isolated or immigrant communities, in maternity homes for the poor or unmarried, and in Aboriginal communities. [2]
A group of Mennonite children, some of whom were probably delivered by unlicensed midwives, pose in an undated early twentieth century photograph.
Source: Mennonite Heritage Centre Archives, Peter G. Hamm Collection, #44-8.
In Manitoba, the speed with which childbirth came under the domain of licensed medical doctors was uneven and was tempered by ethnic politics. This paper examines a specific instance of an attempt to bring medical childbirth to the Mennonite block settlement in South Central Manitoba known as the Mennonite West Reserve. The case of Katharina Thiessen’s prosecution by Morden doctors and the College of Physicians and Surgeons points to the dynamics of making childbirth and illness the exclusive domain of licensed practitioners. In contrast to Adam Scalena’s analysis of the contest between licensed doctors and chiropractors and osteopaths, which argues that economi c motives played a lesser role in Manitoba than in other jurisdictions, Thiessen’s case suggests that the medicalization of childbirth was an economic issue for individual doctors who had a license to practice. [3] The presence of folk remedies, midwives and other purveyors of traditional medicine represented a loss of revenue for them. Doctors also made every attempt to medicalize childbirth by emphasizing their gender and social superiority in order to gain control of the lucrative medical market of the Mennonite West Reserve. Further, Thiessen’s case illustrates how an ethnic group was able resist the intrusion of the doctor, an ethnic outsider in the 1890s, into the private realms of illness and childbirth. Finally, the case of Katharina Thiessen suggests that giving doctors exclusive domain over illness and childbirth was a precarious project in the 1890s. The intervention of ethnic politics forced the College of Physicians and Surgeons to abandon the project of medicalizing childbirth among Mennonites because of the risk of jeopardizing their goals in the province more generally.
The practice of midwifery was based on traditional views of childbirth as a natural process. Midwives relied on their practical experience to guide them as to whether or not they should intervene in the birthing process. Physicians, however, had formal training at medical schools that gave them social esteem and allowed them to project an air of intellectual and practical superiority over midwives. Further, most midwives were female and most doctors were male, and thus, as Judith Leavitt points out, an element of gender-based status differences existed that put men at an advantage over women regardless of skill or education. [4]
Doctors emphasized their superiority over midwives in part because doctors had an economic interest in showing that birthing was a medical process. Wendy Mitchinson’s research has shown that obstetrics was a foot in the door to a larger and much more lucrative family practice. [5] Contact doctors made with a family during childbirth helped to familiarize the family with what physicians had to offer and gave them the opportunity to gain the family’s trust. This in turn led to the possibility of the doctor being called on for other medical concerns of the family. Thus, Mitchinson shows that if a midwife was called instead of a physician to help a birthing woman, she was not only depriving the doctor of his medical fee but also denying him the opportunity for career advancement. [6] Midwives capitalized on this process of familiarization and building trust through birthing practices in the same way physicians did, so major competition between doctors and midwives understandably developed. [7]
Equally frustrating to doctors was that midwives could get away with charging little or nothing for their services because they often had other means of support. Further, in addition to the delivery itself, midwives offered other related services to the family that physicians did not, such as doing chores, preparing meals, and providing after-care to mother and infant. Physicians, however, were forced to charge their patients at least a moderate fee for their services because their profession was their only income. Thus, many people in the community, particularly the poor, chose to rely on the services of a midwife because they seemed to be the “sensible choice.” [8] The economic competition that midwives created in the medical profession was very threatening to physicians and therefore was one motivation for doctors to show that birthing was a medical process, not a natural or social process as it had been thought about traditionally.
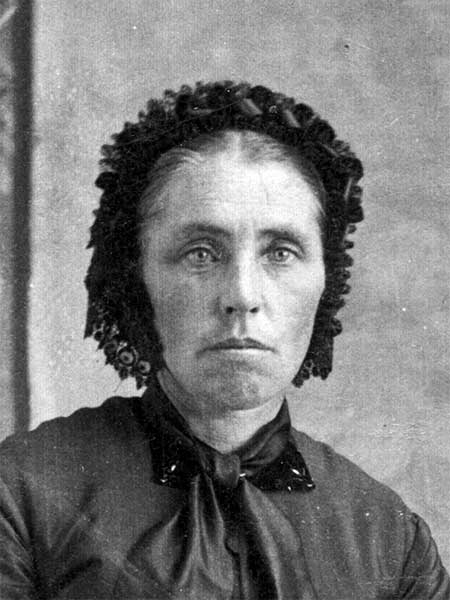
Katharina Born Thiessen (1842–1915) had received training in midwifery, chiropractics, and naturopathy in Prussia before emigrating to North America. She practiced medicine in the West Reserve from 1885 to 1907, after which she continued to sell patent medicines to friends and neighbours.
Source: I. Hildebrand.
Doctors also emphasized their gender and social superiority in order to medicalize childbirth. For example, William Buchan, a late nineteenth century physician, challenged women’s involvement in the birthing process entirely, suggesting that the labouring mother was the only woman that should be involved. He believed that many of the difficulties that women had in birthing could be prevented by disallowing women’s practice of midwifery “unless they are duly qualified.” His statement makes it sound as though he was willing to accept that midwives could provide a valuable service if they were appropriately trained. However, Buchan goes on to ask, “Was any female ever duly qualified? I believe not.” [9] While Buchan’s attitude towards women may not be representative, it does illustrate some important points. First, it showcases the popular nineteenth century belief that men were intellectually superior to women, and shows that gender did play some part in the push for medicalization. If men with a heightened intellect and formal training rather than an untrained female midwife were to assist birthing women, the logic went that the doctor would naturally be able to make birthing more safe. [10]
The role of gender in medicalizing childbirth also shows that status had a part to play in the process. Physicians paid for their training, spent a significant amount of time in medical school, and had to pass examinations in order to become qualified and registered. Midwives, however, generally had made no such time or financial commitments; for the most part remaining uneducated and untrained except for the practical experience they gained by attending numerous births. As Mitchinson points out, physicians felt that having untrained persons doing the job for which they had been formally trained lowered their collective status. [11]
The lack of formal training and qualifications that Buchan discusses above are another reason that physicians wanted to emphasize birthing as a medical process. Many midwives had little or no formal training, which in some cases may have contributed to injury and death of the infant, the mother, or both. Doctors were concerned that birthing mothers got the best treatment available, treatment that they would not receive from untrained midwives. Wendy Mitchinson suggests that physicians were less bothered by midwives that had at least some formal training, because those women would be aware that they should turn a complicated birth over to a trained physician who would have a better chance of saving the lives of the mother and infant. [12] Mitchinson goes on to illustrate the irony of physicians’ serious concerns with midwives’ lack of formal training, in that the obstetric education received by physicians was “substandard.” Medical students received abundant theoretical knowledge through lectures, but witnessed few, if any, real-life births. In fact, many “trained” physicians of the late nineteenth century received their practical experience in obstetrics using a doll and a mannequin. [13] Poor medical training continued to be a problem into the twentieth century, as noted in 1912 by J. Whitridge Williams, professor of obstetrics at Johns Hopkins Medical School. Williams maintained the “average practitioner, through his lack of preparation for the practice of obstetrics, may do his patients as much harm as the much maligned midwife.” [14]
Midwives may have had the practical experience that doctors lacked, but doctors had the scientific knowledge that midwives did not. Paul Starr discusses the impact of trust in science on the medicalization process:
The medical profession has had an especially persuasive claim to authority. Unlike the law and the clergy, it enjoys close bonds with modern science, and at least for most of the last century, scientific knowledge has held a privileged status in the hierarchy of belief. Even among the sciences, medicine occupies a special position. [15]
Medicine’s close ties to science thus had an impact on its perceived authority because of the social value ascribed to scientific research and discovery. However, it was women whom the medical profession had to convince of their superiority over midwives. There were more fundamental reasons than scientific authority that ultimately caused women to put their trust in science. It was scientific knowledge and technology that influenced so many women to abandon midwives for doctors because it brought them practical benefits while giving birth, such as pain relief through anaesthesia and physical aid in labour via forceps. Because birthing women had the authority and power to determine who would help them and what would and would not be done to them or for them during their labour, physicians could not force themselves into birthing rooms by negating the assistance of midwives. It was only when women were convinced that physicians were better suited to assist in labour and delivery that childbirth became medicalized. [16] Access to new medical technology is what helped to convince women that doctors were better suited to care for them during the birthing process than were midwives because of the “progress” that was made when technology and scientific knowledge were applied to obstetrics. [17]
The medical establishment.
Nurses pose on the steps of the Morden Hospital, circa 1910.
Source: Archives of Manitoba, Morden-Hospitals 2, N3783.
One of these technologies, anaesthesia, was and typically is still very important to birthing women. According to Wendy Mitchinson, the lack of training and knowledge regarding anaesthesia may have been a major contribution to midwives’ waning numbers and importance. Once anaesthesia was widely available and proven to be effective, women “began to demand it because of the comfort it could provide” during childbirth as opposed to the comparative pain and suffering that women endured without painkillers. [18] Forceps were also a major contribution of science and technology to childbirth. If applied correctly and used skilfully, forceps could help a complicated birth to progress and could even save the lives of the mother and child. In both of these cases, doctors were the only persons trained to use such technology, so only the patients of medical doctors could reap the benefits, economic or otherwise, of this new technology. [19]
With the introduction of painkillers and forceps, women began to gravitate towards physicians and away from midwives. In fact, Leavitt points out that women seldom chose to revert to the traditional midwife once they had experienced giving birth in the care of a doctor because of the comfort he could provide. Women felt that they were more likely to survive the birthing process if they had a doctor overseeing their labour. [20] By putting their trust in science and technology, women contributed to, or possibly dictated, the medicalization of childbirth.
Despite the development of this more mainstream ideology, Leavitt describes a distinct group of women that she describes as “traditionalist.” [21] This group was typically made up of immigrant women who shared the traditional view that “birth only rarely needed the outside consultation of the medical profession.” Neighbourhood women acted as midwives and did not charge a formal fee, but rather accepted donations or “presents” of two to three dollars for their help. [22]
The practices of Leavitt’s “traditionalist” group closely match the birthing practices of the Mennonite peoples in Manitoba at the turn of the century. Mennonites were a pacifist, German-speaking group who had migrated to Canada in the 1870s in response to military reforms in Russia that threatened their military exemption. Mennonites had a long history of negotiating with governments for special exemptions, usually to ensure the right to practice their pacifist beliefs and to secure the ability to live separate lives. Before arriving in Manitoba, they negotiated with the Canadian government for grants of land in block sections so that they could form their own communities and live apart from the rest of society. [23] As the settlement of Western Canada progressed, the two areas in which they lived in Manitoba became ethnic enclaves that were increasingly surrounded by British and other Western European immigrants.
Living separately from mainstream society was important to the Mennonites; it was thus crucial for the community to be bound together with strong, cohesive bonds. The cooperative birthing and medical practices that developed within the Mennonite community were a reflection of this kinship and communal self-reliance. Often, one or two untrained but knowledgeable women in a given Mennonite community would be designated as community midwives and lay doctors and often remained in that informal but important position long enough to mend many broken bones, to nurse many illnesses, and to deliver many of the next generation of children. [24] Further, specialized birthing and delivery skills and knowledge were passed on from mother to daughter, thus allowing the community to continue to sustain its separation by avoiding outside medical intervention. [25] Royden Loewen has argued that midwives held a respected and valued place within the Mennonite community because of the important practical and ideological niche they filled. Their esteemed role is noteworthy because of the generally patriarchal nature of the Mennonite community; midwives and lay doctors were the only women allowed and encouraged to be in the public sphere by male community leaders. Often midwives and lay doctors were seen to have a special church-ordained gift of medical knowledge that allowed them to provide this essential service to the community. [26] Although these niche roles and the women who filled them were deeply valued by the Mennonite community, they were disdained by the professional medical community that emerged as modernization came to Manitoba.
The Mennonite West Reserve in South Central Manitoba was one of the more densely settled rural areas of the province and the arrival of the railway in the Reserve in the 1880s gave rise to the new railway towns of Gretna, Morden and Plum Coulee. The railway was soon followed by a variety of merchants, lumber dealers, banks, and doctors seeking to profit from the lucrative Mennonite market. In 1892, ten years after the arrival of the railway, Morden businessman and politician Valentine Winkler established the Village of Winkler on the railway tracks near the Mennonite village of Hoffnungsfeld. Located just seven miles East of Morden, Winkler and Morden were soon in heated competition for the business of the Mennonites of the West Reserve.
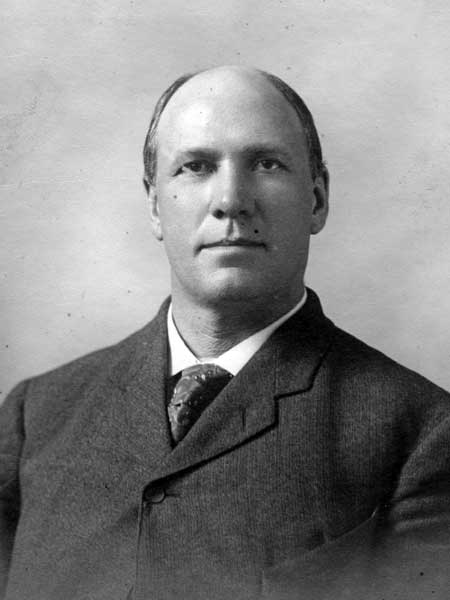
MLA Valentine Winkler (1864–1920) defended Katharina Thiessen from allegations of medical malpractice, and paid her fine levied by the provincial court in 1895.
Source: Archives of Manitoba, Legislative Assembly, 1907–1910.
Trained doctors in the railway towns of the Mennonite West Reserve soon realized that they faced a lively competition from what they broadly categorized as “quacks.” Beginning in the late 1880s a stream of letters was directed to the Manitoba College of Physicians and Surgeons asking them to pursue the prosecution of a variety of unlicensed practitioners. For the individual doctor the main reason for wanting the College to stop midwifery and informal doctors was for personal gain. Dr. Donovan from Gretna reported that there were at least five or six “quacks” practicing in the Mennonite Reserve at the time. Donovan’s problem with a certain Dr. Tyson, probably Katharina Thiessen, was that she was “charging regularly as much as five dollars for consultations.” Donovan complained bitterly to the registrar of the College that nothing was being done to give protection to licensed doctors. [27]
In 1894, doctors B. J. McConnell and F. W. E. Burnham of Morden joined Drs. Donovan and James McKenty of Gretna in the campaign against unlicensed practitioners in the Mennonite reserve. Burnham, in particular, was a persistent and vociferous advocate of prosecution. The theme of economic loss resulting from the presence of lay medicine pervades Burnham’s correspondence with the College’s registrar. In an 1894 letter Burnham claimed the quacks “not only bleed the people of their hard earned money so that when finally they come to a reputable physician they are financially exhausted, but they do actual injury to their patients and I may cite cases where both life and reason have been destroyed.” Burnham claimed that unlicensed practitioners were often “aliens from Minnesota and Dakota who live here a short time reap a rich harvest and suddenly light out to enjoy it elsewhere.” In a later letter that mentions Katharina Thiessen and a Mrs. Bergen particularly, Burnham points out that the Mennonites are faithful in paying for medical services and as a result the two women “take considerable money out of our practice and if there is any way of stopping them I will be glad to assist you.” Burnham believed the College was there to help his practice by eliminating the formidable competition of midwives, naturopaths, and lay doctors. As he puts it in one of his many letters, the main purpose of the College as he saw it was “the protection of the brotherhood.” [28]
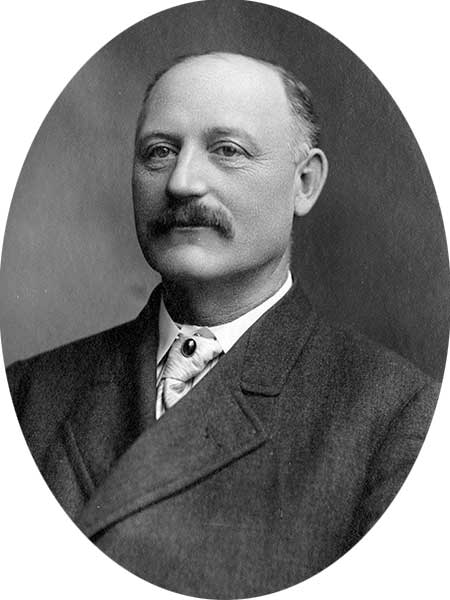
Dr. Benjamin James McConnell (1861–1923) was one of several physicians in southern Manitoba who complained to the Manitoba College of Physicians and Surgeons about “quacks” who were providing unlicensed medical care in the West Reserve. After practicing in Morden and Winnipeg, he entered provincial politics as an MLA, serving from 1907 to 1914.
Source: Archives of Manitoba, Legislative Assembly, 1907–1910.
Many of the “quacks” in the Mennonite Reserve do appear to have been short-lived opportunists, but Katharina Thiessen, a Mennonite midwife who practiced in the Winkler area and who seemed to fill the niche role described by Loewen, proved to be a more resilient challenger to the doctors’ ambitions. Thiessen was a Mennonite immigrant from Russia who at age eighteen had traveled to Prussia to train as a midwife. She married a farmer in Russia and the couple had one son. They migrated to Peabody, Kansas in 1874 where she practiced medicine and her husband farmed. By the 1880s, the Thiessens were attracted to the free homesteads of the Prairies and, in 1885, they moved to Manitoba and settled in a Mennonite village near the site of the later Village of Winkler. [29] Thiessen not only assisted at childbirth in area villages but also performed trauma surgery and traditional medicine. She indicates in a letter to the College that she also had learned to administer a new treatment for cancer, a skill she had learned during a special trip to Cincinnati, Ohio. [30]
F. W. E. Burnham’s constant badgering finally forced the College of Physicians and Surgeons to pursue Katherina Thiessen and another Mennonite doctor, Mr. Abram Hiebert, in the Morden courts. Although it seems doctors in Gretna and Morden were able to convince witnesses to appear in the cases of the non-Mennonite unlicensed practitioners, it was much more difficult to find Mennonite witnesses that would testify against one of their own. When Katharina Thiessen was first charged in April 1895 the witness that had agreed to testify ended up offering testimony that worked against the doctors’ case. The witness claimed that Thiessen had treated his eyes and some time later, he had given her a gift of eight dollars. As the Morden lawyer acting for the College ruefully notes in his correspondence to the registrar, the presiding magistrate once had his horse treated by someone whom he had given a two-dollar gift. The magistrate took his own experience as sufficient precedent to dismiss the charges against Thiessen. The lawyer notes that it would be beneficial to have someone who spoke German working on the doctor’s behalf because it was proving difficult to gather evidence because of the intense opposition to the prosecutions in the area. The second attempt to prosecute unlicensed Mennonite practitioners in the courts also failed because in the case of one defendant the witness that had been arranged for backed out at the last minute. Thiessen’s case at the same trial date had to be set aside because the constable had not served her with a proper summons, causing the magistrate to again dismiss the case. [31]
The evidence that was ultimately presented against Thiessen was that she had assisted in the delivery of a baby using forceps where the baby died within ten hours of the procedure. Legal counsel for the College of Physicians and Surgeons pointed out during the preparation of the case that the evidence being offered possibly constituted malpractice and might very well diminish sympathy for the accused, but it was not sufficient grounds for prosecution under the Medical Act. Counsel pointed out that evidence would need to establish that the accused had no license, had performed medical surgery or midwifery, and had received, “gain or hope of reward.” [32]
The 1871 Medical Act, part of the new Province of Manitoba’s first laws, outlawed unlicensed midwifery and gave free reign to the Provincial Medical Board, all of whom were trained doctors, to determine qualifications for licensing in those cases where the applicant had not graduated from an approved medical college. The law that succeeded this first Act, the Medical Act of 1886, established the College of Physicians and Surgeons and added the economic caveat that licensing was required for midwifery or other practices of medicine or surgery if there was “gain or hope of reward.” [33] As legal counsel pointed out to both the College and Dr. Burnham, evidence would have to be brought forward to show that Katherina Thiessen and other lay practitioners were not only practicing, but also charging for their services.
“A number of quacks.”
Files of the Manitoba College of Physicians and Surgeons are filled with complaint letters such as this 1894 example from Morden physician Frederick Burnham (1870–1955).
Source: Archives of Manitoba, College of Physicians and Surgeons, P6746.
After a few false starts, Hiebert was convicted and then on 11 June 1895, Katharina Thiessen was also convicted in Morden court and fined fifty dollars. The conviction of the two Mennonite practitioners drew immediate opposition from Mennonites. The contest between Thiessen, the Morden doctors and the College soon involved Valentine Winkler, the German Lutheran founder of the Village of Winkler and an MLA who represented the Mennonite area. The contest pitted ethnic political clout against the medical establishment. Burnham reported that there was “considerable feeling in the Reserve as a result of the cases and the people blame us for it.” [34] Although most Mennonites shunned direct participation in politics they were not averse to pressuring their non-Mennonite representatives to vigorously pursue their interests. The Morden lawyer acting on behalf of the College and the Morden doctors reported that Valentine Winkler, the MLA for the Mennonite area, had appeared in court to pay the fine on behalf of Katharina Thiessen where he had also indicated he was on his way to Winnipeg to introduce an amendment to the Medical Act that would exempt Mennonites from its provisions. [35]
The Morden newspapers and the ethnic Mennonite and German Press immediately weighed in on the issue. The Morden Monitor, a political rival of Valentine Winkler, believed the issue was really a masked form of trying to boost the fortunes of the new railway town of Winkler just down the track. The Monitor claimed, “a great dust is being made over these medical cases by designing persons in order to boom Winkler at the expense of Morden.” [36] The Monitor was against a separate law for Mennonites countering that if an exemption was given to Mennonites the Icelandic and French communities would be next. The Monitor argued that there should be one law for midwives and doctors for the entire province. The Nordwesten, a German language paper read by many Mennonites, supported its ethnic readership but pursued the economic argument, claiming it was “utterly impossible for poor people to pay high fees charged by the medical profession.” [37] The Mennonite German language paper, the Rundschau, offered greater insight into the reasons for the quick action of the area’s MLA. An anonymous writer to the paper appealed for support for the Mennonite practitioners from the ethnic community. The writer reminded readers that Thiessen was known and loved throughout Southern Manitoba as an experienced doctor. The writer sought to establish Thiessen’s credibility and value to the community and thought it regrettable “that a woman who had done immeasurable good among her coreligionists was pursued and persecuted in this way because of envy.” The clearest indication that Mennonites considered the prosecutions an ethnic issue came in the writer’s indictment that the law seemed to be on the side of the “English doctors.” [38]
The ethnic dimensions of the issue were not lost on those advising the College. In a lengthy legal opinion Hough and Campbell acknowledged the unique situation of Mennonites as an ethnic group whose traditional form of medical care was being threatened. Hough and Campbell reminded the College that “it appears that Mr. Winkler M.P.P. has been asked to represent the feelings of a large section of the Mennonite people who regard Mr. Hiebert as a physician and who also think Mrs. Thiessen is qualified for the practice of midwifery,” and that “Mennonites are to some extent a people of themselves.” [39]
Although there was some understanding of the Mennonite position, the vigour and method by which Valentine Winkler was pursuing the issue caused grave concern to the College that went considerably beyond the problem of quack doctors in Southern Manitoba. Legal counsel pointed out that the issue had broader implications for establishing doctors’ status in the rest of the province. While counsel believed that the legislature would not have time to consider an amendment to the Medical Act such as that suggested by Valentine Winkler, there was
a great deal of “Patron” jealousy of the professions lately in the legislature, in fact it is somewhat pronounced …. A bill therefore to repeal the clauses forbidding medical practice without registration might have strong support though we think it would fail of passing. [40]
The correspondence between legal counsel and the College of Physicians and Surgeons suggest that support for granting doctors the exclusive right to practice medicine and to deliver babies in the province was not general and that the organized efforts that were being mounted by the Mennonites to protect their own medical practitioners might well jeopardize the greater goal of licensing medical practice throughout the province. As alluded to in the legal opinion, the College had already recognized the danger and responded to Valentine Winkler’s threat. According to Burnham, Valentine Winkler had told him that at a meeting between the College and legislators, the College had claimed that the prosecutions of Thiessen and Hiebert had been entirely the work of Morden doctors, not the College, and had offered to refund the fines imposed on the two lay practitioners. [41] Further, the College’s legal counsel, Hough and Campbell, concurred with the decision by the College to stop further prosecutions under the Manitoba Medical Act in the Mennonite Reserve. They believed that “the implied promise given to Mr. Winkler by you and others for the Executive that if his bill were not put forward the two persons in question would not be further prosecuted by or at the insistence of the Council was not only wisely given but under the circumstances was called for.” [42]
Clearly the attempt by Valentine Winkler to address the issue of medicalizing birth and illness, which was upsetting his ethnic constituents, had put at risk the move of doctors to reserve those domains for formally trained and properly licensed doctors throughout the province. The College and Valentine Winkler forged a deal that would see the former stop prosecuting unlicensed Mennonite midwives and lay doctors in exchange for the latter’s withdrawal of the threat to introduce an amendment to the Medical Act. The pursuit of individual gain that was behind the Morden and Gretna doctors pursuit of prosecution had threatened public support for restricting medical practice and birth to licensed doctors. This reality was most clearly illustrated by legal counsel’s final advice to the College. Hough and Campbell suggested the College remind Dr. Burnham “that no professional man is supposed to have any chartered rights. The Medical Act is for the benefit of the public and not for that merely of the physician.” [43]
F. W. E. Burnham was forced to concede defeat although he and the other doctors continued to pursue prosecutions, including further actions against both Thiessen and Hiebert. In the case of the two Mennonite practitioners, however, the College always found ways of honouring its 1895 commitment. Katharina Thiessen continued to practice in the Winkler area for another fifteen years although her husband’s ill health increasingly took up her time after he suffered a stroke in 1907. She retired from her practice in 1909 and died in 1915 of a massive stroke. While Burnham was prepared to accept the College’s decision, he could not understand why they had not limited their promise to the practice of midwifery. In his letter after the compromise he conceded, “it would be satisfactory if the practice of these Mennonites was strictly limited to midwifery and I think that this is the easiest solution of the trouble. If the College of Physicians & Surgeons would give these people to distinctly understand that they were violating the law but that they would be permitted to practice midwifery they would be satisfied.” [44]
The prosecution of Katharina Thiessen offers new insights into the dynamics of the process of the medicalization of childbirth and illness and particularly how doctors in Manitoba pursued that process. Mitchinson’s observation that doctors’ attempts to wrestle childbirth away from midwives were driven to a large extent by economics seems to apply to the doctors involved in the case of Katharina Thiessen. Individual doctors, while believing their training could offer superior health care to the community, were motivated more by the difficulties of competing with midwives and traditional healers for the community’s available financial resources. Doctors in Gretna and Morden had difficulty understanding the cautious approach taken by the College, which felt more keenly the responsibility of balancing the need to demonstrate that restricting medicine to licensed doctors was in the public’s interest on the one hand, with the desire of doctors to have their competition swept away on the other.
Mennonites saw the licensing of doctors as an intrusion of “English” society on a domain they firmly believed to be within the bounds of community, family and religion and marshalled ethnic politics to press for exemption from the laws of the land, as they had so often before. Valentine Winkler’s role was clearly that of leveraging the precarious support for giving to doctors’ privileges that were not yet widely supported by society to gain the exemption sought by his constituents. The contest put the College of Physicians and Surgeons in a difficult position. While the College was charged with furthering the project of placing medical practice and childbirth firmly under the regulations of the Manitoba Medical Act, the risk of losing the cause entirely was real. The compromise allowed both the recognition of ethnic sensibilities and the larger project of bringing childbirth and illness under the domain of licensed and educated doctors. The problem would disappear when Mennonites began to train their own licensed doctors and the benefits of trained medical care became apparent to them. Licensed doctors soon made their home in Winkler but it would take until 1925 when Dr. C. W. Wiebe, one of their own, set up practice in Winkler that the role of the midwife and lay doctor diminished in the villages around Winkler. [45]
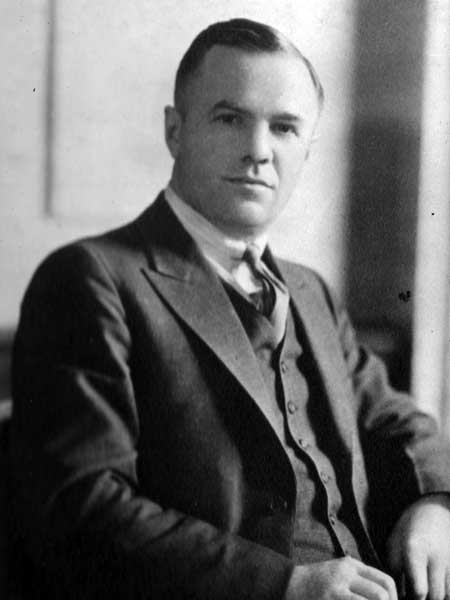
Dr. Cornelius W. Wiebe (1893-1999) began a medical practice in Winkler in 1925. By the time he retired in 1978, he is thought to have delivered over 6,000 babies.
Source: Archives of Manitoba, Legislative Assembly 1932-1936.
1. Mitchinson, Wendy, The Nature of Their Bodies: Women and Their Doctors in Victorian Canada. Toronto: University of Toronto Press, 1991, p. 167.
2. Mitchinson, Wendy, Giving Birth in Canada, 1900–1950. Toronto: University of Toronto Press, 2002, p. 70.
3. Scalena, Adam, “Defining Quackery: An Examination of the Manitoba Medical Profession and the Early Development of Professional Unity,” Journal of the Canadian Chiropractic Association, 2006, vol. 50(3), p. 210.
4. Leavitt, Judith W., Brought to Bed: Childbearing in America, 1750 to 1950, New York: Oxford University Press, 1986, p. 39.
5. Mitchinson, The Nature of Their Bodies, p. 170.
6. Ibid.
7. Mitchinson, Giving Birth in Canada, p. 33.
8. Mitchinson, The Nature of Their Bodies, pp. 168–69.
9. Ibid., p. 170.
10. Ibid., p. 163.
11. Ibid., p. 172.
12. Ibid., p. 171.
13. Ibid., pp. 172–73.
14. As quoted in Leavitt, p. 63.
15. Starr, Paul, The Social Transformation of American Medicine, New York: Basic Books, 1982, p. 4. See also Mitchinson, Bodies, p. 163.
16. Mitchinson, The Nature of Their Bodies, p. 162; Leavitt, p. 62.
17. Mitchinson, The Nature of Their Bodies, p. 172.
18. Ibid., p. 179.
19. Leavitt, p. 47.
20. Ibid., p. 58.
21. Ibid., p. 78.
22. Ibid., p. 79.
23. There are a number of different arrangements that various communities made to remain apart from the mainstream. See Graydon F. Snyder, Health and Medicine in the Anabaptist Tradition: Care in Community, Valley Forge: Trinity Press, 1995, p. 135.
24. Vogt, Esther Loewen, “Horse and Buggy Midwife,” in Women Among the Brethren, ed. Katie Funk Wiebe, Hillsboro: Board of Christian Literature of the General Conference of Mennonite Brethern Churches, 1979, p. 75.
25. Vogt, p. 77.
26. Loewen, Royden K., “‘The Children, the Cows, My Dear Man and My Sister’: The Transplanted Lives of Mennonite Farm Women, 1874–1900,” Canadian Historical Review, 1992, vol. 73(3), p. 365.
27. Letters from Donovan to J. S. Gray, Registrar, undated, Correspondence, 1886–1894, College of Physicians and Surgeons, Archives of Manitoba, P6746.
28. F. W. E. Burnham to J. S. Gray, Registrar, 16 July 1894, Correspondence, 1886–1894, College of Physicians and Surgeons, Archives of Manitoba, P6746. F. W. E. Burnham was a young doctor at this time, having graduated from the Manitoba Medical College in 1894. He later practiced in Winnipeg and during the First World War served in the Balkans where he was a decorated surgeon. He died in 1957 when the sanatorium at the Halcyon Hot Springs near Castlegar, B.C., which he and his wife had directed, burned to the ground. See “Dr. F. W. E. Burnham 1872-1957: A Life of Strange Adventure,” Manitoba Medical Review, 1966 vol. 46(9), pp. 569-570.
29. Bergen, Shirley, “Dr. Katherina Born Thiessen: A Woman Who Made a Difference,” Mennonite Historian 1997, vol. 23(3) p. 8. See also John Dyck, “Hoffnungsfeld: Community and Phenomenon,” in Adolf Ens, Jacob E. Peters and Otto Hamm,eds. Church, Family and Village: Essays on Mennonite Life on the West Reserve, Winnipeg: Manitoba Mennonite Historical Society, 2001, p. 209.
30. Mrs. A. K. Thiessen to the College, undated, Correspondence, 1895–1897, File R-Z, Manitoba Archives, P6746. See also Shirley Bergen, “Life of Mrs. Dr. Thiessen (nee Catherine Bornn) 1842–1915,” unpublished manuscript, Mennonite Heritage Centre, Vol. 5028, File 7.
31. H. McConnell to J. S. Gray, 29 April 1895 and Burnham to the College, 5 June 1895, Correspondence, 1895–1897, File A-C and D-L, College of Physicians and Surgeons, Archives of Manitoba, P6746.
32. Hough and Campbell to Gray, 2 March 1895, Correspondence, 1886–1894, file D-L, College of Physicians and Surgeons, Archives of Manitoba, P6746.
33. “An Act Relating to Medical Practitioners in this Province,” 34 VIC, CAP 26, 3 May 1887, art. 7 and “An Act Respecting the Profession of Medicine and Surgery,” 49 VIC, CAP 31, 28 May 1886, art. 31.
34. Burnham to Gray, 5 June 1895, Correspondence, 1895–1897, File A-C, College of Physicians and Surgeons, Archives of Manitoba, P6746.
35. H. McConnell to Gray, 12 June, 1895, Correspondence, 1895–1897, File M-Q, College of Physicians and Surgeons, Archives of Manitoba, P6746.
36. Morden Monitor, 27 June 1895.
37. As quoted in the Morden Monitor, 27 June 1895.
38. Mennonitische Rundschau, 3 July 1895.
39. Hough and Campbell to College, 20 June 1895, Correspondence, 1895–1897, file D-L, College of Physicians and Surgeons, Archives of Manitoba, P6746.
40. Ibid.
41. Burnham to Gray, 24 June 1895, Correspondence, 1895–1897, file D-L, College of Physicians and Surgeons, Archives of Manitoba, P6746.
42. Hough and Campbell to College, 20 June 1895, Correspondence, 1895–1897, File D-L, College of Physicians and Surgeons, Archives of Manitoba, P6746.
43. Hough and Campbell to J. S. Gray, 20 June 1895, Correspondence, 1895–1897, File, D-L, College of Physicians and Surgeons, Archives of Manitoba, P6746.
44. Burnham to the College, 2 July 1895, Correspondence, 1895–1897, File A-C, College of Physicians and Surgeons, Archives of Manitoba, P6746.
45. Werner, Hans, Living Between Worlds: A History of Winkler, Winkler: Winkler Heritage Society, 2006, 108ff. and Mavis Reimer, Cornelius W. Wiebe: A Beloved Physician, Winnipeg: Hyperion Press, 1983.
Page revised: 30 August 2014