by Leah Morton
Winnipeg, Manitoba
|
Many Manitobans over the age of sixty have memories of the recurring polio epidemics that struck the province in the mid-part of the century. Some of the more enduring memories associated with epidemic polio include woollen hot packs, admonitions from parents to avoid swimming pools, and iron lungs. These images and memories, though, are largely specific only to the last two epidemics. The first recorded polio epidemic in Manitoba occurred in 1928 and the last in the summer and fall of 1953. In that twenty-six year span, which I characterize as the epidemic era, there were six large-scale outbreaks of polio in Manitoba. The epidemic era ended only with the introduction of the vaccine created by American Jonas Salk.
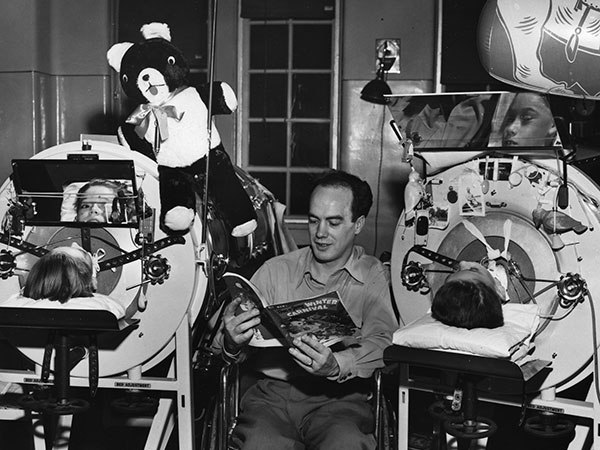
Iron children. Long-term confinement to an iron lung was a common result of diaphragm paralysis caused by poliomyelitis. Here, John Bryant reads to children as part of the Merry Menders Club at the King George Hospital, 9 December 1953.
Source: University of Manitoba Archives & Special Collections, PC018-A81-012-056-5375-024.
The way polio was approached and treated changed throughout the epidemic era. This article focuses on the changing nature of the approaches to polio, concentrating in particular on attempts to contain the disease, the role of nurses, and patient management. Responses to the earliest epidemics, in 1928 and 1936, centred on medical attempts to control the disease through the use of serums and nasal sprays. Although finding something to minimize the effects of the disease continued to be a priority of the medico-scientific community, patient management and the role of nurses became increasingly important, particularly after 1941. A review of the changing approaches to polio management helps make sense of the incurable epidemic viral disease that caused so much anxiety and dread in Manitoba, but that has largely been forgotten since the advent of the successful polio vaccines.
While Manitoba was not the only province to contend with multiple polio epidemics, it was arguably the hardest hit region, with epidemics developing in 1928, 1936, 1941, 1947 and 1952. The era of epidemic polio in Manitoba concluded with the massive 1953 epidemic. In 1928, there were 434 confirmed cases of polio in Manitoba. [1] The majority of those affected were children under the age of five. The tendency for polio to affect young children, coupled with the resulting paralysis, is why it was known popularly for many years as infantile paralysis. [2]
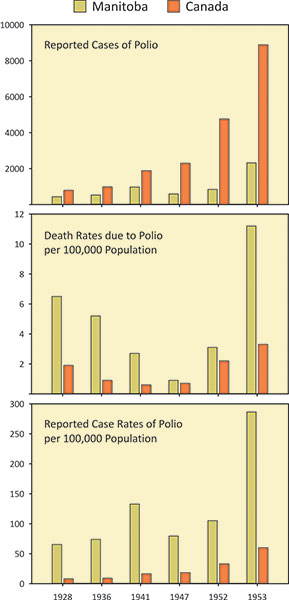
Statistics from 1928 to 1953 illustrate how Manitobans were affected by poliomyelitis disproportionately to other Canadians.
Source: C. J. Rutty “Do Something!...Do Anything! Poliomyelitis in Canada, 1927-1962” PhD dissertation, University of Toronto, 1995: 396-398.
With each successive epidemic in Manitoba, polio became more virulent, and it began to affect older individuals. In 1941, 969 Manitobans were affected, leading to a case rate of 132.7 per 100,000 population. [3] While these numbers are quite high, they do not compare to what happened in 1953. Manitoba experienced a particularly large outbreak in 1952; so, polio was not expected to be a concern in the coming year. By November 1953, however, over 2,300 Manitobans had been stricken with polio, with a case rate of 286.4 per 100,000. To make matters worse, many contracted bulbar polio, which paralysed the breathing muscles, leading not only to the enduring iron lung images, but also to an uncommonly high death rate. [4]
Throughout the epidemic era, people worried constantly about polio. Even though the mortality rate was usually quite low, polio engendered great anxiety. Dr. Oswald Day of the Children’s Hospital in Winnipeg was intimately involved in the pre-war epidemics. “I do not believe that there is any disease that can frighten people so profoundly,” Day wrote in a 1929 article in the Canadian Medical Association Journal, “as poliomyelitis. In Winnipeg last year, it incited a terror among them much like that caused by the air-raids during the war.” [5] To have made such a comparison only a decade removed from the horrors of the Great War is eye-opening. The lack of a cure and the inability to predict or contain an outbreak were part of the reason why polio evoked such serious apprehension.
However troubling, those issues were not the only reasons why polio was so feared. That had more to do with the target demographic and the results of a bout of polio. Until the 1950s, polio attacked young children most frequently; in 1928, over half of the individuals stricken with polio in the city of Winnipeg were 10 or under, whereas only 3.1 percent were over the age of 25. [6] Its early symptoms—a general malaise, headache and stiff joints—mirrored those of so many common ailments. To think that a child could progress from generally not feeling well to paralysis in a matter of hours or days was genuinely disconcerting.
The perils associated with polio were already well known in North America by the time it first appeared in epidemic form in Manitoba. Polio first appeared in Vermont at the turn of the century, but it was the enormous outbreak in New York State in 1916 that established polio as a feared disease against which the usual public health measures, such as quarantine and an emphasis on cleanliness, proved ineffective. [7] By the time that epidemic subsided in December 1916, “in New York City alone there were 8,900 cases and 2,400 deaths,” establishing polio as a fearsome, incurable disease that targeted and paralyzed young children. [8]
In July 1928, the confidence with which the medical community faced polio belied the fact that very little was actually known about the disease. American scientists had been studying the epidemiology of polio since the turn of the century, yet little had been discovered in terms of control or prevention. Manitoba doctors seemed to believe they could effectively manage the disease and by mid-August 1928, the Medical Research Committee of the University of Manitoba was on the case. The Faculty Medical Research Committee (MRC), made up of professors and physicians from the Manitoba Medical College, was a standing committee that met when necessary. On 17 August 1928, the members of the MRC were summoned for an emergency meeting. At the meeting, Dr. F. T. Cadham, Professor of Bacteriology, outlined “the situation respecting the outbreak of poliomyelitis in Winnipeg, which [was] beginning to approach the epidemic stage.” [9] This, and subsequent MRC meetings, set the tone for the way the first recorded polio outbreak was handled in Manitoba.
The MRC believed they could control the growing epidemic with something known as poliomyelitis serum, or convalescent serum. The idea that a serum might be effective in controlling a disease was not new. Health researcher Christopher Rutty, in his examination of medical and official responses to polio in Canada, suggests that serums were popular in the treatment of diphtheria and were often used to “minimize the severity of measles, scarlet fever and whooping cough.” [10] Within this context, it is not surprising that the use of a convalescent serum, that was made from the blood of individuals who had supposedly recovered from polio, and reputed to lessen the effects of the disease if administered before the onset of paralysis, became the MRC’s main focus.
The provincial Department of Public Health and Public Welfare supported this initiative and it was at the Minister’s request that the MRC became involved in the battle to contain and control the growing epidemic. The provincial Board of Health decreed that the MRC “should be authorized to prepare a convalescent serum for use in the treatment of poliomyelitis, and that the investigation of the present epidemic as to the etiology, clinical course, and treatment should be undertaken” by the MRC. Additionally, “all matters with the scientific aspect of the problem” were delegated to the MRC. [11] A poliomyelitis subcommittee, made up of a number of notable Winnipeg doctors, including Dr. Bruce Chown, was struck and they turned to the growing epidemic.
The MRC was careful not to refer to the serum as a cure, but its centrality in the fight against polio in 1928 shows how much confidence was placed in its efficacy. By the end of August, over 100 cases had already been reported and it was clear that Winnipeg was in the midst of an epidemic. The MRC wasted little time in setting out its plan. Backed financially by the province, the committee gained permission from the municipal health authorities to observe patients at the King George Hospital. They also drafted permission forms for potential blood donors, asked Dr. Cadham to produce convalescent serum, and set out the parameters regarding which cases would be suitable for serum treatment. [12] Once these preliminary measures were put in place, the MRC asked the research lab to establish day and night services for the creation and distribution of the serum.
The MRC’s emphasis on the serum necessitated finding suitable blood donors, a task which proved to be difficult. It relied heavily on the two urban daily newspapers, The Winnipeg Tribune and the Manitoba Free Press to find potential donors. Front-page advertisements with the headline “Blood Urgently Needed” were placed in both dailies and the ads stressed that there was no risk to the potential donor. [13] Because the blood had to be from someone who had previously contracted polio, it was difficult to find enough donors. The Winnipeg Health Department had a list of such individuals, which it shared with the MRC, indicating that although this was the first recorded outbreak, polio had definitely been present in Manitoba prior to 1928. Despite problems with the list, including their inability to find some of the individuals, the MRC was able to secure approximately 100 donors, many of whom donated blood more than once. Although the MRC claimed to have a sufficient amount of donor blood to make the serum, they were clearly worried about a shortage, requesting serum from Toronto, Edmonton and British Columbia in early September. [14]
Despite not having any evidence of the efficacy of the serum, the MRC went to great lengths to provide serum to doctors and patients. The provincial government could not officially recommend its use as it was “still in the experimental stage”; however, the province and the MRC strongly believed in the serum and were committed to making it available to any physician who requested it. The MRC went to great lengths to have it distributed to as many cases as possible. Physicians would personally deliver serum to any suspected cases within a one-hundred-mile radius of Winnipeg, and for rural cases, “assistance was received from officials of the railway companies in several ways. In some instances conductors took personal charge of the serum, and in one or two instances trains were stopped specially at points of delivery.” [15] The centrality of the serum to the battle against polio is undeniable as considerable amounts of time and money were clearly spent on its creation and dissemination in the province.
The MRC’s evidence in 1928 for the efficacy of the serum is doubtful and, by 1936, convalescent serum had been characterized as harmless, and ineffectual. However, the overwhelming desire to find something that could alleviate the effects of polio remained strong throughout the whole of the epidemic era. This is evident in the drive to develop a special nasal spray during the 1936 epidemic and the development of an improved serum in 1953.
With the surge in the number of reported cases of polio in the summer of 1936, hopes were pinned on a nasal spray. The spray, which was reported to have “shown favourable results in the southern United States,” was made by mixing picric acid with sodium alum. It was recommended by the provincial Department of Health as part of “its efforts to halt the Infantile Paralysis epidemic.” [16]
The questionable nature of the nasal spray did not seem to deter the provincial board of health. Despite the fact that the spray turned people’s noses yellow, and that it had been previously tested only on monkeys, the Department used provincial public health nurses and doctors to promote its use as a preventative, although they refrained from positioning it as a cure. It recommended that the spray be made by a “competent druggist” and administered, of course, by a physician. Step-by-step instructions were included, however, in the 15 August edition of the Free Press, presumably for worried parties who possessed both sodium alum and picric acid!
Nasal sprays quickly fell out of fashion in the North American fight against polio, but preventatives in general did not. Nasal sprays had been touted as possible preventatives based on the belief that “the portal of entry of the poliovirus was the olfactory nerves of the nose.” [17] Although the spray used in Manitoba during the 1936 epidemic was harmless, other nasal sprays were more damaging, and quickly discontinued. [18]
Serums, though, were used in the fight to contain polio throughout the whole of the epidemic era in Manitoba. In 1941, the province experienced a dual epidemic of polio and encephalitis. In July of that year, it became clear to the Department of Health and Public Welfare that an epidemic was imminent, and a medical Advisory Committee was quickly assembled. The Advisory Committee was comprised of several doctors who had been involved with the MRC in 1928, including Bruce Chown, O. J. Day and F. T. Cadham. [19] By 1941, opinion was divided as to the efficacy of the serum. Even though the Advisory Committee “could see no immediate effect from the serum,” it was still given to each suspected case. [20] The Advisory Committee acknowledged that “much difference of opinion [existed] as to its effect;” however, the provincial bacteriologist, Dr. Cadham was once again asked to make the serum, because many in the medical field and general public continued to believe that its use “contributed to the low morality” associated with polio. [21]
Convalescent serum continued to be used, despite questions about its usefulness, because it gave the appearance that the medical profession was able to do something to combat the mysterious disease that frightened Manitobans. For all the work that went into studying the symptoms and clinical course of the disease, there was little that doctors could actually do for a person suffering from polio. Indeed, as the Advisory Committee conceded, “…besides the serum, only symptomatic treatment was given.” [22] Physicians did what they could to mitigate the painful headaches, stiffness and nausea that signalled the onset of polio, but beyond that, they were stymied.
Although neither the convalescent serum nor the spray was particularly useful, the medical community continued, right until the end of the epidemic era, to search for a prophylactic that might lessen the effects of polio. In 1952 and 1953, hopes were pinned on something known as gamma globulin. Gamma globulin, the part of the blood rich in antibodies, was made by utilizing “sophisticated blood fractionating techniques” resulting, apparently, in an “immune serum thirty times more concentrated than convalescent serum.” [23] Although globulin efficacy was unproven, the mounting panic over the severity of the 1953 epidemic, coupled with limited supplies and the tendency of the press to tout gamma globulin as a cure, led to a political controversy over its distribution. Gamma globulin was in short supply in Canada, and the federal government strictly controlled and monitored its supply. When rumours arose that gamma globulin could be obtained on the black market, CCF leader Lloyd Stinson castigated the ruling Liberal party for misleading the public in desperate times. [24] The Winnipeg Trades and Labour Council also demanded answers from Paul Martin, the federal Minister of Health and Welfare. Martin asked the Advisory Committee to reiterate to the TLC that gamma globulin was reserved for those who needed it most, not those who could afford to buy it privately. [25]
A number of factors, including the way it was reported in the Winnipeg daily newspapers, precipitated the furor over gamma globulin. Physicians and government officials were careful not to present gamma globulin as a cure or failsafe preventative against polio, but the language used in the media may have convinced the general public otherwise. Both the Free Press and the Tribune, for example, referred multiple times to gamma globulin as an “anti-polio serum” and at one point, the Free Press lamented that there was not enough gamma globulin available for mass immunizations against the disease. [26]
The language implying that gamma globulin would prevent polio further confused an already volatile situation, and played on the emotions of citizens desperate to save their children from the ravages of polio. One father, whose daughter had been stricken by the disease, tried in vain to purchase a dose of gamma globulin, even offering to pay forty dollars for the vial. [27] The publicity surrounding gamma globulin, combined with the media representations, made it the latest in a long line of preventatives that Manitobans hoped in vain would help shield their families from polio.
Despite the continued search for some sort of preventative, the whole dynamic of polio treatment shifted dramatically in 1941. This shift led to a focus on the treatment and aftercare of patients, particularly those who suffered residual paralysis, and it greatly affected the work performed by nurses during epidemics. This change occurred right in the middle of the 1941 epidemic, and was precipitated not by the realization that the serum was ineffective but by the groundbreaking work of Elizabeth Kenny, an informally trained Australian nurse.
Sister Kenny demonstrates her therapy for polio patients to another nursing sister in a hospital at Queensland, Australia, 1939.
Source: State Library of Queensland, John Oxley Library, D1-5-89.
Prior to 1941, nursing was not a concern to those leading the battle against polio in Manitoba. The aftercare of the patients was barely an afterthought for the MRC in 1928 and 1936. During the 1928 epidemic, the MRC published in the Winnipeg daily newspapers information on topics such as the symptoms, possible causes and epidemiology of polio; the news items were later reprinted as part of the province’s official report on the epidemic. The MRC’s material concerned with the treatment of polio focuses exclusively on the use of the serum. Nursing the polio patients is not mentioned at all in that article, or anywhere in the report. [28] Tellingly, the journal The Canadian Nurse simply republished the MRC’s informational articles in 1929, without adding anything about nursing polio patients.
The focus on finding a preventative rendered nursing and patient management almost invisible in the medical and public discourses during the early epidemics, but the orthodox treatment of polio-related paralysis also limited the scope of nursing care. Prior to 1941, the mainstream management of patients with paralysis hinged on two principles: complete bedrest, and immobilization. The MRC firmly suggested that “rest is the sheet anchor in the treatment” of paralysis. So that no one might assume rest meant simply taking it easy after a bout with polio, they reiterated that “this means rest in bed.” [29] The second aspect of the pre-1941 treatment—the immobilization of affected limbs—was done through splinting. The MRC subscribed to the widely accepted belief that splinting was necessary to “prevent overstretching of the paralyzed muscles, and to prevent the occurrence of deformity.” [30] Once the affected limb was splinted, the patient, usually a young child, was strapped to a Bradford frame, which was little more than a long piece of wood with cloth or metal straps that could be secured around the arms and legs to prevent movement. Within the prevailing medical orthodoxy of splinting and immobilization, there was little that nurses could do for polio patients, other than general upkeep such as bathing and feeding. This does not, however, mean that nurses were completely removed from the care of polio patients at all. Mary Shepherd was a young RN who was working as a private duty nurse when the head nurse at the King George Hospital contacted her in September of that year. She wanted to know if Shepherd was available to help out for a month or two. As this coincided with the height of the epidemic, it is reasonable to assume the increased number of patients necessitated the head nurse’s hiring another nurse. According to Shepherd, nurses in 1928 followed strict techniques when working with patients in isolation, but it does not seem as if there was anything specific they had to do for those suffering from polio-related paralysis. [31]
The 1941 polio epidemic represents a watershed in the context of nursing and patient management in Manitoba. The polio epidemic was unique in that it coincided with an outbreak of encephalitis, or sleeping sickness. The “twin epidemic” brought increased attention to the province, as members of the international medical community and the federal department of health and welfare came to Manitoba to observe the unfolding outbreaks. [32] One of the international visitors was Sister Elizabeth Kenny, and it was her ideas about paralytic polio that not only revolutionized patient management, but also transformed the role of nurses from peripheral to central in the day-to-day care of those suffering the effects of polio.
Elizabeth Kenny, by 1941, was well known to those intimately involved in the fight against polio. Although not a formally trained nurse, Kenny had a great deal of experience working with polio patients, first in her homeland of Australia, and later in North America. Through her work with polio sufferers in Australia, Kenny developed some very specific ideas about the management of paralysed muscles and advocated a treatment regimen that differed completely from the accepted mainstream methods of splinting, rest and immobilization. Kenny postulated that the affected muscles were in a state of spasm, akin to a severe cramp. These spasms made the surrounding muscles flaccid, rendering the limb immobile. Because of the pain associated with the spasm, patients would lose “mental awareness of the flaccid muscles” causing them to become “alienated from their brain control.” [33]
The Kenny method focused on relieving both the spasm and the muscle alienation in ways that specifically contradicted the prevailing orthodoxy. Indeed, Kenny believed that rest and immobilization did more harm than good to patients trying to recover use of their affected limbs. The first step was the application of fomentations, or hot packs. Strips of wool blankets were torn up and then placed into boiling water. When they were hot enough, but not so hot as to burn the patient, they were placed on the affected limb, until cooled. This was to be repeated several times a day in order to relieve the painful spasm associated with paralytic polio. Muscle alienation was dealt with through stretching the muscles and moving the joints through a number of controlled exercises and by teaching the patients to consciously relax healthy muscles. [34] The treatment was to begin as soon as the patient passed out of the acute phase of the disease, usually within a week or two after the onset of symptoms.
By the time officials in Manitoba knew they were in for another epidemic in 1941, Dr. Bruce Chown, then Superintendent of the Children’s Hospital in Winnipeg, decided to pay a visit to Kenny’s Minneapolis clinic, despite her well-known clashes with medical authorities. Chown was a rational, open-minded physician, but he was also frustrated. This was the third epidemic to hit the province in thirteen years, and there was little he could do to prevent the devastation it caused his community. Believing that the “whole disease is in need of reassessment,” Chown was sufficiently impressed with the outcome of Kenny’s work that he invited her to visit Winnipeg to further demonstrate her work. [35] Kenny accepted the invitation and arrived at the Children’s Hospital in the middle of the epidemic. Undaunted, she set to work, and spent two weeks teaching the physicians, nurses and physiotherapists how to make the hot packs and manipulate the affected limbs and muscles.
A Winnipeg physician uses the Kenny method to treat a young polio patient, July 1953.
Source: University of Manitoba Archives & Special Collections, PC018-A81-012-056-5375-017.
The transformation engendered by the Kenny method was profound: previously relegated to the sidelines, nurses suddenly had a main role to play in the treatment of polio patients. Nurses were responsible for making and changing the hot packs, sometimes every hour, and while physiotherapists were supposed to perform the exercises, the lack of therapists in Manitoba meant nurses took on this role as well. Polio nursing was undergoing a sudden and dramatic transformation. Not mentioned at all in the 1928 provincial report, nurses suddenly became central to the management of polio.
Chronic nursing shortages were an unintended consequence of the changes engendered by the implementation of the Kenny method. The hot packs, combined with the muscle manipulation prescribed by Kenny, meant that in each of the epidemics after 1941, there were never enough nurses. This inexorable need for nurses became clear almost immediately in 1941. In each subsequent year, the ad-hoc committees set up to deal with the epidemics brought nursing to the fore, publicly calling for assistance from nurses.
The circumstances surrounding the massive 1953 epidemic led to a particularly contentious nursing shortage. Manitoba had been hit by a sizable epidemic in 1952, with just under 1000 cases reported. The established pattern suggested that polio would be minimal in 1953. However, by July of that year, it was clear that Manitoba was in for another epidemic. At the height of the new epidemic, it was not unusual to have a hundred cases reported in a week, or in a single weekend. [36] To make matters worse, many of the cases were of the bulbar variety, and young adults rather than children seemed to be the more susceptible. The beginning of the school year was delayed by several weeks, and the Air Force was asked to perform “mercy flights” to bring more iron lungs to the city. In total, over 2,200 cases were reported from July to November 1953.
The implementation of the Kenny method was not the only change nurses had to deal with in the later part of the epidemic era. The increasing frequency of bulbar polio in 1953 led to more labour-intensive and technology-based work for nurses. Bulbar polio “damaged cranial nerves in the spinal cord, severely affecting breathing and swallowing” [37] and respirators, commonly known as iron lungs, were needed to keep these people alive for weeks, months, years, and in some cases, decades. [38] The unprecedented number of bulbar polio patients during the 1953 epidemic had serious implications for the nurses who were responsible for their care. The literature for nurses tending iron lungs suggested that they were basic machines that could be operated with very little training. “All respirator equipment is basically simple, and the nurse only requires a short period of personal examination of the machine and an explanation from someone who has operated one to comprehend…” how to operate an iron lung. [39]
This discourse underestimated the enormous amounts of technical skill, knowledge and teamwork that went into nursing a patient in an iron lung. Even in optimal conditions, tasks such as bathing the patient, administering enemas or changing catheters needed to be performed with the patient still inside the respirator. Small portholes in the machines, which operate on the principle of negative pressure, gave nurses limited access to the patients’ bodies, however, and their arms could be placed in the portholes only when the bellows of the machine were up, making these complex tasks all the more difficult. Nurses also needed to know how to keep the machines running during emergencies, although this technological expertise is downplayed in the literature as well. Hospitals rarely suffered power failures, nurses were told, and besides, there was a simple handle that could work the machine manually! [40]
This upbeat take on the manual operation of an iron lung can be juxtaposed to an incident that occurred at the King George Hospital at the height of the 1953 epidemic. Mary Shepherd, hired on temporarily at the King George during the 1928 epidemic, was by 1953, the Superintendent of Nursing. [41] Shepherd’s experience with a power outage at the King George Hospital in 1953, when 99 patients were in iron lungs tells a much different story from what appeared in The Canadian Nurse. According to Shepherd, it took three people to keep just one iron lung working manually. One person had to unplug the machine and work the pump manually, taking care not to breathe the patient too slowly or quickly. The second person had to stand on the side to read the pressure gauges to make sure the first person was pumping at the correct pace, and the third person had to be stationed at the patient’s head to suction their saliva and mucous, because they couldn’t swallow on their own. Shepherd’s nursing staff, along with medical personnel from all the other wards, worked to keep 99 iron lungs operating in complete darkness for four hours, until the power was restored. Clearly, it was not an easy task. As Shepherd recalled, “it was bedlam.” [42]
Nursing shortages had become common towards the end of the epidemic era, and staffing was problematic, particularly in terms of the nurses’ service and remuneration. The time-consuming, labour-intensive, and technical work nurses performed on the polio wards in 1953 certainly contributed to the issue. Yet the way the 1953 Polio Advisory Committee (PAC), the ad-hoc committee of medical professionals and government officials set up in 1952, and again in 1953, depicted the growing outbreak in the press also factored into the representation of nurses throughout the epidemic. The PAC, in order to prevent panic over the escalating outbreak, used the press continuously to reassure the public that the chances of contracting polio were low. [43] The Free Press reported Manitoba’s first new polio cases of 1953 in late June, but the 39 cases reported as of 2 July 1952 were brushed off by officials as “hangover cases” from 1952 and it was reiterated that there was “no cause for deep anxiety.” [44]
Juxtaposed to these efforts to downplay the rising number of cases were the constant pleas, on behalf of the PAC, for nurses to volunteer at the King George Hospital, where the majority of the patients were hospitalized. The call for nurses started almost immediately after the first cases were reported. At the beginning of July, a letter was sent to over 700 “inactive nurses in the Greater Winnipeg area” asking them to “register for a refresher course on polio.” The course was presented as a cautionary, pro-active measure, for although “medical authorities do not expect an epidemic” nurses needed to be up to date on unspecified “new treatment methods.” [45] The calm tone of the first calls quickly dissipated; only two weeks later the seemingly benign request for nurses to update their knowledge turned into an “urgent” appeal for nurses by the Polio Advisory Committee. [46] By 20 July, the city felt it had to close down its child health centres in order to free up nurses, and nurses from the Armed Forces were reassigned to Winnipeg hospitals. The ambiguities in the way the growing epidemic was presented by the PAC and the press may have contributed to the response of inactive and potential nurses. If the outbreak were not serious, as officials claimed, why were they so desperate for nurses?
Dedication to service was one of the main causes of the contentious feelings between nurses and officials in 1953. By November of that year, the epidemic had subsided, but controversy over the nurses had not. In November 1953, Lillian Mackenzie, the Director of Public Health Nursing for the City of Winnipeg, sent a letter to Dr. Roper Cadham, the Deputy Health Officer and spokesperson for the PAC. Cadham had asked for information about “the response of the City Health Department Nursing Division to requests for assistance during the 1953 poliomyelitis epidemic.” Mackenzie replied that out of the 48 nurses employed by the City, 39 had volunteered either at the gamma globulin clinic or on the hospital wards. The majority of those who chose not to volunteer were either pregnant or had family members who were seriously ill, and had been advised not to volunteer. [47] Despite Mackenzie’s prompt reply, the PAC clearly felt that nurses, particularly those employed by the city, had shirked their duty during the worst of the outbreak and Mackenzie was once again asked to justify her nurses’ actions during the epidemic.
In a series of questions sent to Mackenzie in March 1954, the PAC pointedly suggested that the majority of City nurses had taken their vacations during the height of the outbreak, and that they had tried to avoid working on the polio ward of the King George by volunteering to staff the clinic that administered the gamma globulin serum to contacts of confirmed polio cases. Mackenzie, in an adamant bid to show how useful her nurses had been, answered the questions sent to her in a straightforward, but meaningful way. She countered the PAC’s contention by noting that one nurse spent her holidays on the wards of the King George, another rearranged her holidays so as to work on the polio wards and four others who did take their holidays during the outbreak did so because immediate family members were sick, and needed their attention. [48]
One of the main sticking points the PAC focused on was remuneration. During the epidemic, the PAC press releases often mentioned that nurses would receive a bonus of an extra $12 for each five days worked. [49] Nurses were vilified during the epidemic, too, for not working unless they were paid accordingly. Doctors were publicly recognized for “working around the clock” and “internes” for “acting as nurses”, but nurses, it seemed, needed to be persuaded with a monetary bonus on top of the “special nurses’ salary” they were already receiving in order to ease the “critical problem” of the nursing shortage.” [50] Almost a year after the epidemic subsided, the question of pay remained controversial. Apparently, some nurses who were temporarily employed at the King George were inadvertently paid twice for their overtime hours. In March 1954, the City of Winnipeg’s municipal health committee sent a letter to the city’s Director of Public Health Nurses, Lillian Mackenzie, demanding to know why none of her nurses who had agreed to work on the polio wards had reported this “obvious duplication.”
While Mackenzie countered that the duplication was not, in fact, obvious, the questions raised by the PAC seemed to be rooted in gendered ideas concerning women and nurturing, nursing work. Historically, women were expected to perform nursing-type work, particularly in the face of moments of disaster, war and medical emergencies. During the 1918 influenza outbreak, for example, the mayor of Ottawa publicly reminded women, that “nursing the flu victims was their ‘duty’ when the city was critically short of qualified nurses.” [51] Nurses in 1953 expected to be paid accordingly for their work, even though the PAC saw them as volunteers, and this may have exacerbated the tension between health authorities and nurses at an already stressful time.
In Manitoba, the epidemic era lasted more than twenty-five years. During this time, approaches to the multiple polio epidemics that hit the province were not static. During the earliest outbreaks, attempts to control and contain the disease emphasized experimental serums and sprays, rather than caring for patients. Although the urge to medically-manage the disease did not dissipate, as indicated by the emphasis in 1953 on gamma globulin, the successful introduction of the Kenny method in Manitoba led to an important shift, namely the growing emphasis on patient care and nurses. The Kenny method, combined with the massive outbreak in 1953, particularly the high number of bulbar cases, put extra pressure on nurses in Winnipeg. Nurses clearly rose to the occasion, even in very trying circumstances; however, their technological expertise in caring for all polio patients, and particularly those in iron lungs, flew in the face of the discourse concerning nurses as feminine voluntary caregivers. While the 1953 epidemic may have left Manitobans with enduring images and memories, it is important to consider the changing nature of polio in Manitoba by examining the epidemic era as a whole.
Gee, that doesn’t hurt! Linda Spence of Portage la Prairie received her first Salk polio vaccination at the Local Health Unit on 21 April 1955. Dr. Joseph Gonty, head of the Unit, administered the vaccination with nurse Rose Mushynski assisting.
Source: Portage Collegiate Archive, Yosh Tashiro Fonds.
1. C. J. Rutty “Do Something!… Do Anything! Poliomyelitis in Canada, 1927–1962.” PhD dissertation, University of Toronto, 1995, p. 397.
2. Polio has gone through several name changes. Prior to the 1930s, it was mainly known as infantile paralysis. The correct terminology is poliomyelitis, and although it is often referred to as such in the scientific and medical literature, physicians, researchers and the press mainly used “polio.” This is the term that will be used in this article.
3. Rutty, p. 396.
4. Rutty, p. 398. Polio death rates were generally quite low in Canada, hovering in the 0.5 to 2.0 per 100,000 range. In Manitoba in 1953, this rose dramatically to 11.2, matched only by a rate of 10.7 in Alberta the same year.
5. O. J. Day “Poliomyelitis in Manitoba in 1928” Canadian Medical Association Journal 21 (November 1929), pp. 554-558.
6. Mary McKenzie, A. T. Cameron and A. J. Douglas “The Distribution of Cases in the Manitoba Epidemic of Poliomyelitis, July–October 1928” in the Report on the Poliomyelitis Epidemic in Manitoba -1928, Winnipeg: Great-West Life Assurance Company, 1929, p. 25.
7. Naomi Rogers, Dirt and Disease: Polio before FDR, New Brunswick: Rutgers University Press, 1993.
8. Ibid., p. 11.
9. Minutes, Meeting of the Medical Research Committee, 17 August 1928. File 10.2.2[2], Faculty Medical Research Committee, Research – Correspondence, minutes, reports 1926–1928, Neil John McLean Library.
10. Rutty, p. 41.
11. Letter to Dr. C. R. Gilmour, Chairman, Medical Research Committee, from Dr. Montgomery, Minister of Public Health and Public Welfare, 31 August 1928. File 10.2.2[2], Faculty Medical Research Committee, Research – Correspondence, minutes, reports 1926–1928, Neil John McLean Library.
12. Minutes, Meeting of the MRC, Thursday, 30 August 1928, File 10.2.2[2], Faculty Medical Research Committee, Research – Correspondence, minutes, reports 1926–1928, Neil John McLean Library.
13. Minutes, Meeting of the MRC Poliomyelitis Sub-committee, Tuesday, 4 September 1928, File 10.2.2[2], Faculty Medical Research Committee, Research – Correspondence, minutes, reports 1926–1928, Neil John McLean Library.
14. C. R. Gilmour and A. T. Cameron, “The organization of the work concerned with the preparation and distribution of convalescent serum and the investigation of its action during the Winnipeg epidemic of poliomyelitis, 1928”, in Report on the Poliomyelitis Epidemic in Manitoba – 1928 by the Medical Research Committee of the University of Manitoba, Winnipeg: The Great-West Life Assurance Company, 1929, p. 13.
15. Ibid., p. 18.
16. “Antiseptic being used in Boissevain District makes noses go yellow” Winnipeg Free Press (hereafter WFP), 15 August 1936, p. 3.
17. Rutty, p. 106.
18. See Chapter 3 of Rutty’s dissertation for a more in-depth analysis of the scientific discourse surrounding nasal sprays and problems related to their use.
19. F. W. Jackson, “Introduction,” Poliomyelitis and Encephalitis Manitoba, 1941: A symposium arranged by the Department of Health and Public Welfare of the Province of Manitoba, pp. 2-5.
20. J. D. Adamson and Sara Dubo, “A Clinical Study of Acute Poliomyelitis, Manitoba 1941”, in Poliomyelitis and Encephalitis Manitoba, 1941: A symposium arranged by the Department of Health and Public Welfare of the Province of Manitoba, pp. 19-34.
21. Ibid., p. 32.
22. Ibid., p. 33.
23. Rutty, pp. 235-236.
24. “Stinson: Polio Shots being Sold”, Winnipeg Tribune (hereafter WT), 21 August 1953, p. 9.
25. “Canadian Polio Serum not for Sale, says Govt” WFP, 19 August 1953, p. 2.
26. See for example: “Anti-Polio Serum Seen Here Shortly”, WFP, Thursday, 9 July 1952, p. 3; “Anti-Polio Use Extended”, WFP, 24 July 1953, p. 6; “Anti-Polio Serum Here”, WT, 13 July 1953, p. 3; “Marketing of Anti-Polio Serum dubbed ‘Perfectly Legitimate’”, WFP, 5 August 1953, p. 3; “Gamma Globulin Lacking for Mass Immunization”, WFP, 17 August, 1953, p. 3.
27. “Marketing of Anti-Polio Serum dubbed ‘Perfectly Legitimate’”, WFP, 5 August 1953, p. 3.
28. “Appendix III”, in the Report on the Poliomyelitis Epidemic in Manitoba – 1928 by the Medical Research Committee of the University of Manitoba (Winnipeg: The Great-West Life Assurance Company, 1929), p. 79.
29. Ibid., p. 81.
30. Ibid.
31. Mary Shepherd interview, 1988. Winnipeg General Hospital Nurses Alumni fonds “Nurses and their Work: Oral Histories of Nursing in Winnipeg, 1920–1940” Archives of Manitoba Tape C901 Side B.
32. F. W. Jackson, “Introduction”, Poliomyelitis and Encephalitis Manitoba, 1941: A symposium arranged by the Department of Health and Public Welfare of the Province of Manitoba 2-5, p. 4.
33. A. E. Deacon, “The Treatment of Poliomyelitis in the Acute Stage”, in Poliomyelitis and Encephalitis Manitoba, 1941: A Symposium arranged by the Department of Health and Welfare of the Province of Manitoba. Reprinted in Canadian Public Health Journal 33(6), pp. 38-41 (June1942).
34. Ibid., p. 40.
35. Bruce Chown, “The Newer Knowledge of the Pathology of Poliomyelitis,” in Poliomyelitis and Encephalitis Manitoba, 1941: A Symposium arranged by the Department of Health and Welfare of the Province of Manitoba. Reprinted in Canadian Public Health Journal 33(6), pp. 36-37 (June 1942).
36. “Week-end polio cases total 95”, WFP, 4 August 1953, p. 1.
37. Lynne Dunphy “‘The Steel Cocoon’: Tales of the Nurses and Patients of the Iron Lung, 1929–1955”, Nursing History Review 9, p. 30 (2001).
38. Mary Shepherd interview, 1988. Winnipeg General Hospital Nurses Alumni fonds “Nurses and their Work: Oral Histories of Nursing in Winnipeg, 1920–1940” Archives of Manitoba Tape C901 Side B. Shepherd states that some bulbar patients were still in iron lungs at the Princess Elizabeth (now the Riverview) hospital.
39. Barbara Montizambert, “Nursing Care of a Patient in a Respirator,” The Canadian Nurse 50(6), pp. 461-463 (June 1954).
40. Montizambert, p. 462.
41. “Seven More Cases of Polio Reported”, WT, 21 July 1953, p. 1.
42. Mary Shepherd interview, 1988. Winnipeg General Hospital Nurses Alumni fonds “Nurses and their Work: Oral Histories of Nursing in Winnipeg, 1920–1940” Archives of Manitoba Tape C901 Side B.
43. “Doctor hits polio epidemic panic: statistics show accidents the greatest killer”, WFP, 22 July 1953, p. 3.
44. “Polio total up by five cases in two weeks”, WFP, 27 June 1953, page 1; “11 polio cases in week hikes province total to 39”, WFP, 2 July 1953, p. 3.
45. “RNs sign up for refresher polio course,” WFP, 3 July 1953, p. 3.
46. “Wading pools unwise now polio committee reports,” WFP, 16 July 1953, p. 1.
47. Letter from Lillian Mackenzie to Dr. Roper Cadham, 24 November 1953, Committee on Health, Pack File H 1492(5), City of Winnipeg Archives.
48. Lillian Mackenzie, memo re: Public Health Nurses, 29 March 1954, Committee on Health, Pack File H 1492(5), City of Winnipeg Archives.
49. “33 more stricken in polio epidemic”, WFP, 20 July 1953:3; “Week-end polio cases total 95”, WFP, 4 August 1953, page 1; “Polio kills two more in Winnipeg”, WFP, 5 August 1953, p. 1; Mary Shepherd interview, MA.
50. “Week-end polio cases total 95”, WFP, 4 August 1953, p. 1.
51. Linda Quiney, “‘Filling the Gaps’: Canadian Voluntary Nurses, the 1917 Halifax Explosion, and the Influenza Epidemic of 1918”, Canadian Bulletin of Medical History 19 (2), page 362 (2002).
Page revised: 16 June 2020